
By: Ryan King, originally published June 22, 2026, The New York Post Golf fans attending the third round of the US Open at Shinnecock Hills Saturday were left stunned when an airplane buzzed the course towing an advertisement promoting obtaining abortion pills by mail. The ad was paid for by Mayday Health, a Massachusetts-based nonprofit dedicated to highlighting the…
The post Abortion pill advertisement at US Open leaves golf fans appalled: ‘Gross and divisive’ appeared first on Cincinnati Right to Life.

By: Amy O’Donnell, originally published June 11, 2026, Society of St. Sebastian For nearly fifty years under Roe v. Wade, abortion was treated as a constitutional right deeply embedded in American law, politics, education, and culture. Organizations like Planned Parenthood aggressively promoted it, especially in low-income and minority communities. Meanwhile, pro-life advocates worked incrementally to save…
The post When Protecting Life Loses Its Heart appeared first on Cincinnati Right to Life.

By: Nancy Flanders, originally published May 15, 2026, LiveAction.org A recent post on X regarding maternal mortality has gone viral, but the post uses a source from nearly two years ago that has already been debunked. Despite this, the misinformation is now making the rounds on social media and has racked up more than 8.7 million views. Yet,…
The post Why a viral tweet about maternal mortality shouldn’t be taken as fact appeared first on Cincinnati Right to Life.

By: Calvin Freiburger, originally published June 5, 2026, LifeSiteNews.com The Trump administration Food and Drug Administration (FDA) has finally begun its review of the data on abortion pill harms, more than a year after the move was promised to frustrated pro-lifers. In May 2025, the Trump administration promised to review abortion pill data, but a year without…
The post Trump FDA finally begins abortion pill review after pressure from pro-lifers appeared first on Cincinnati Right to Life.

By: Mary Rose, originally published June 5, 2026, The Loop/Zeale News. Parents of children with Down syndrome took to X June 4 to share stories of love and advocacy, responding to a viral post by YouTuber Jesse Ridgway in which he announced he and his wife aborted their unborn child after learning the baby had…
The post “The happiest people on Earth’: Down syndrome families flood social media after YouTuber aborts baby due to Down syndrome diagnosis appeared first on Cincinnati Right to Life.

By: Elise Winland, originally published June 4, 2026, The Loop/Zeale News Chloe Cole, a 21-year-old detransitioner, urged Congress during an emotional June 3 hearing to ban gender “transition” procedures for children, alleging that doctors lied to her family and left her with irreversible physical and emotional harm. Cole — who began “transitioning” at age 12…
The post Detransitioner Chloe Cole urges Congress to ban gender ‘transition’ procedures for minors during heated Senate hearing appeared first on Cincinnati Right to Life.

By: Dan Hart, originally published May 27, 2026, The Washington Stand A startling new study has revealed that the vast majority of online abortion drug vendors are shipping the pills to women whose unborn children are past the point of 10 weeks’ gestation, in violation of the FDA’s federal safety limit. The report, released by the…
The post Study: 64 Online Abortion Pill Vendors Ignore 10-Week Gestational Limit appeared first on Cincinnati Right to Life.
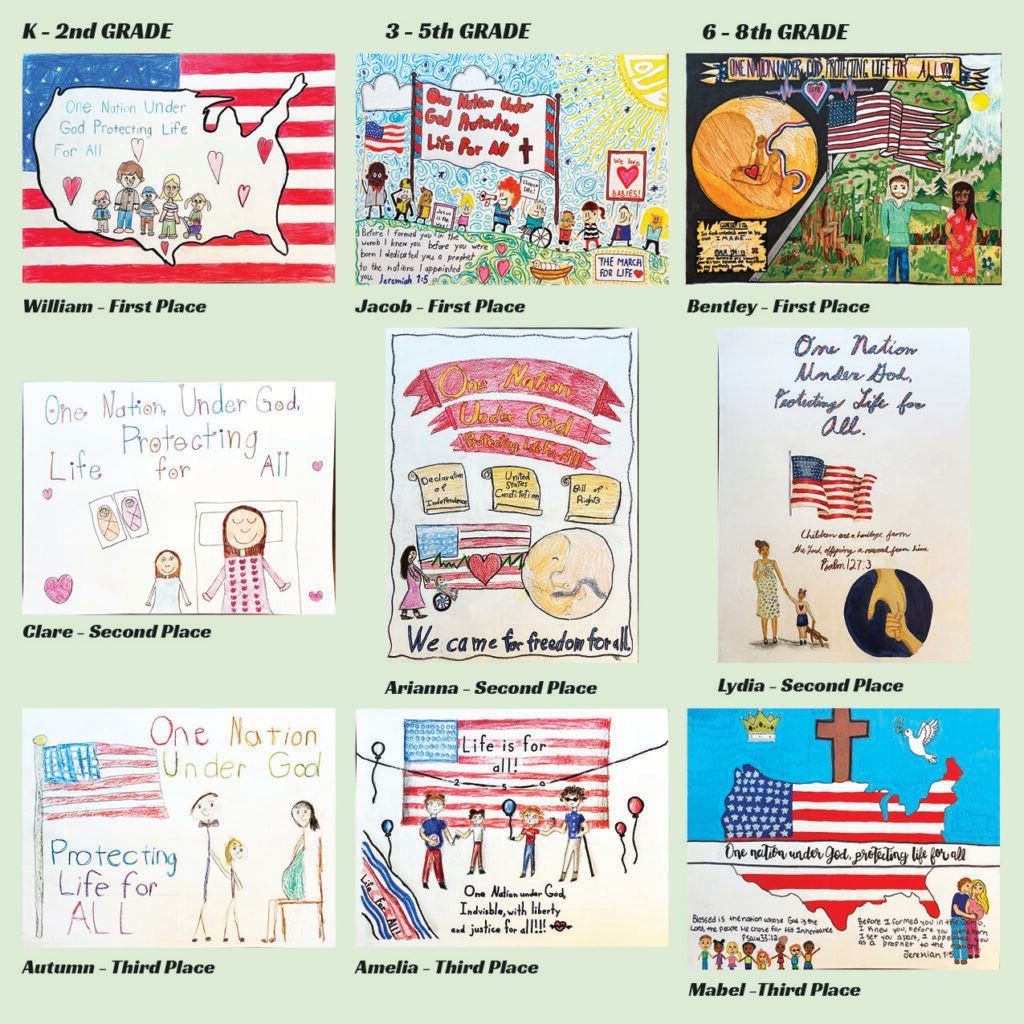
Congratulations to the winners of this year’s Pro-Life Poster Contest!! We received 510 submissions! The students very brilliantly depicted this year’s theme “One Nation Under God, Protecting Life For All.” Here are the 20261st, 2nd, & 3rd Place Winners: Thank you to all those who participated!!
The post Announcing Cincinnati Right to Life’s 2026 Poster Contest Winners! appeared first on Cincinnati Right to Life.

From Right to Life Action Coalition of Ohio State Senators are HESITATING on SupportingSub. H.B. 485, Enact the Baby Olivia Act IMMEDIATE ALERT to CALL and EMAILThursday, May 28Friday, May 29Monday, June 1 CALLSenate Education Committee Members Sen. Andrew Brenner, Chair 614-466-8086 ohiosenate.gov/andrew-o-brenner Sen. Louis Blessing, III, Vice Chair 614-466-8068 ohiosenate.gov/louis-w-blessing-iii Sen. Al Cutrona 614-466-8285 ohiosenate.gov/al-cutrona Sen. Steve…
The post ACTION ALERT! Call and Email State Senators! appeared first on Cincinnati Right to Life.

By: Calvin Freiburger, originally published May 21, 2026, LifeSiteNews WASHINGTON, D.C. (LifeSiteNews) — Top Republicans on the U.S. House Oversight Subcommittee on Delivering on Government Efficiency are seeking information from Planned Parenthood affiliates around the country on the abortion giant’s abortion practices and work “transitioning” gender-confused children. The Daily Signal reported that the committee chairman, Republican Reps. Tim…
The post Republicans demand answers from Planned Parenthood on abortions, ‘gender transitions’ for minors appeared first on Cincinnati Right to Life.
